Beyond Cholesterol: What You Need to Know About Apolipoprotein B's Crucial Role in Cardiovascular Risk.

Introduction and Editor's Tangent: Welcome to this multi-part series where we delve into the intricate topic of cholesterol (also known as lipids) and its connection to cardiovascular risk assessment. Let's kick off this series with a focus on apolipoprotein B (apo-lipo-protein), technically referred to as apolipoprotein B100. For the sake of simplicity, we'll refer to it as apoB moving forward.
Before you decide where this article relates to you-- Unless you're a newborn 👶🏼, age doesn't exempt you from these concerns. Disease processes such as atherogenesis and atherosclerosis, which can lead to heart attacks and strokes, can begin to develop as early as ages 10-14. It's crucial to note that the risk of cardiovascular disease is multifactorial—many factors contribute to one's risk. Apolipoprotein B and cholesterol represent just a couple of the many factors involved.
First, lets get on the same page about cholesterol. What is cholesterol and why do we need it?
Gist: Cholesterol is a waxy, fat-like substance that's found in all the cells in your body. In addition to your liver, every cell in your body has the ability to produce cholesterol. It is essential to life.
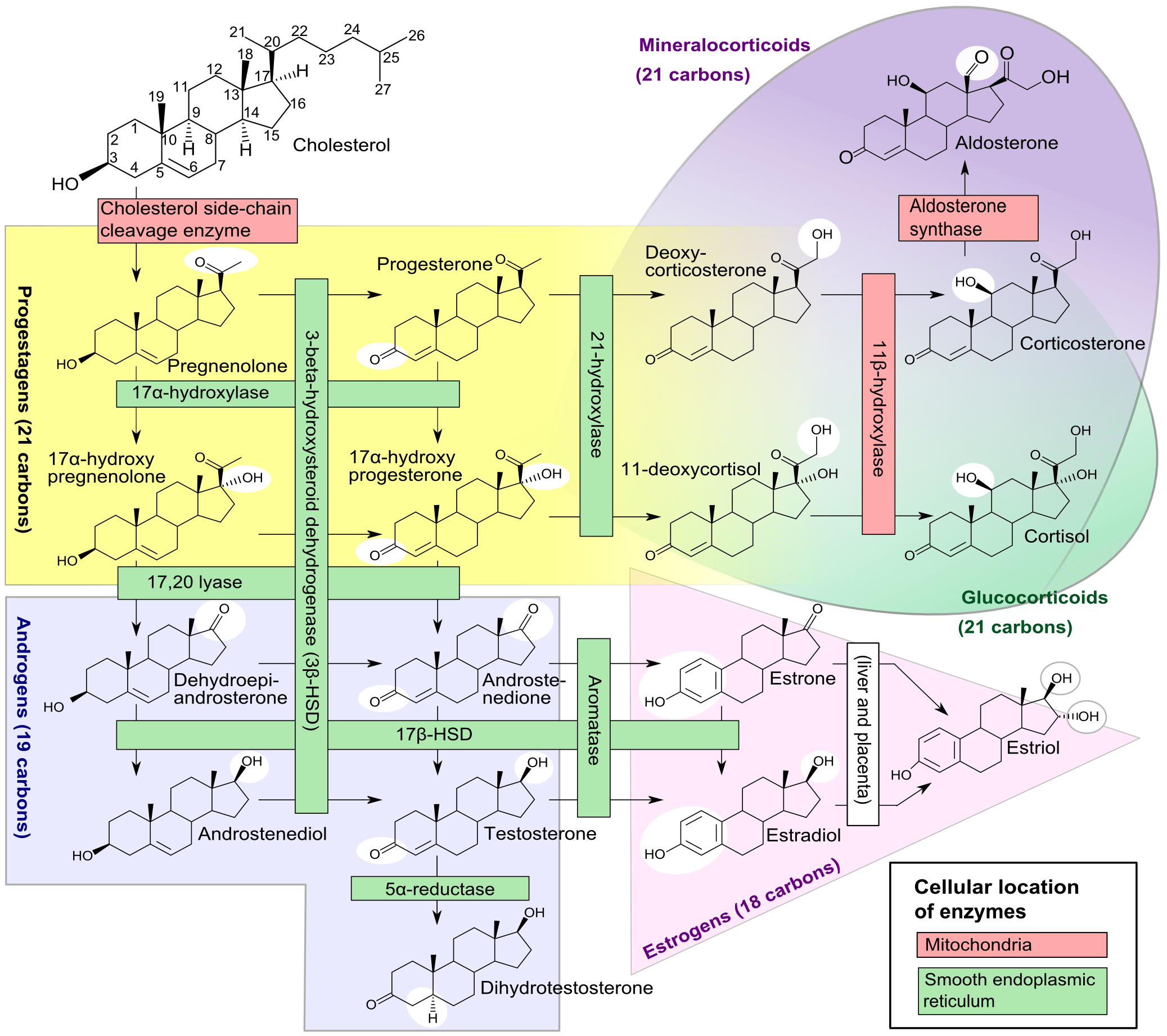
Nitty-Gritty: Cholesterol plays a vital role in our bodies. It contributes to the structure of cell membranes, aids in the production of bile acids necessary for digestion in the intestine, and facilitates the body's synthesis of vitamin D. Additionally, it enables the body to produce certain hormones, including cortisol, progesterone, estrogen, and testosterone.
How is your cholesterol measured?
Gist: A cholesterol panel, also known as a lipid panel or profile, is a blood test that measures the levels of different types of lipids, in your blood. You typically see these categories:
- Total cholesterol (TC)
- Low-Density Lipoprotein Cholesterol (LDL-C)
- High-Density Lipoprotein Cholesterol (HDL-C)
- Triglycerides (TG)
- Non-HDL Cholesterol (Non-HDL-C)
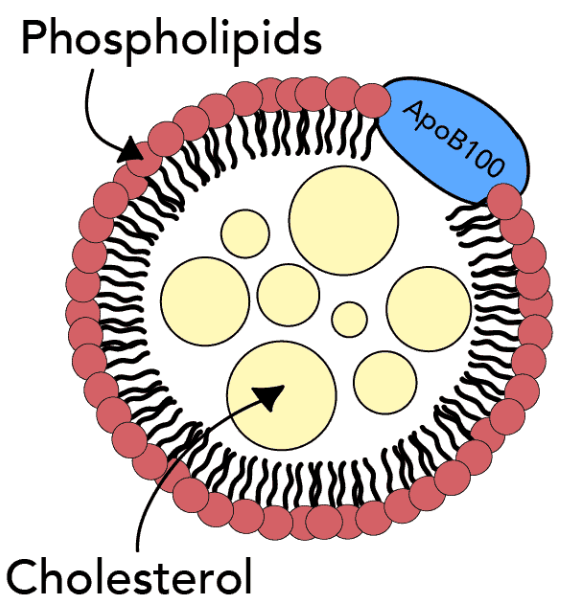
Nitty-Gritty: Cholesterol needs to be transported to various parts of your body through your bloodstream. This transportation is facilitated by proteins, which serve as vehicles🚗. The combination of cholesterol and protein (with some triglycerides in mixed in there as well) forms a particle known as a lipoprotein, such as low-density lipoprotein (LDL), high-density lipoprotein (HDL) and so on.
Cholesterol + Protein = Lipoprotein Particle
However, the levels outlined on your blood test results are a reflection of the concentration (in units of millimole per litre, abbreviated mmol/L) of each category, not the number of particles.*Keep this in mind, we will apply this fact below.
What is the difference between the types of cholesterol (i.e. lipoproteins) listed above all about then?
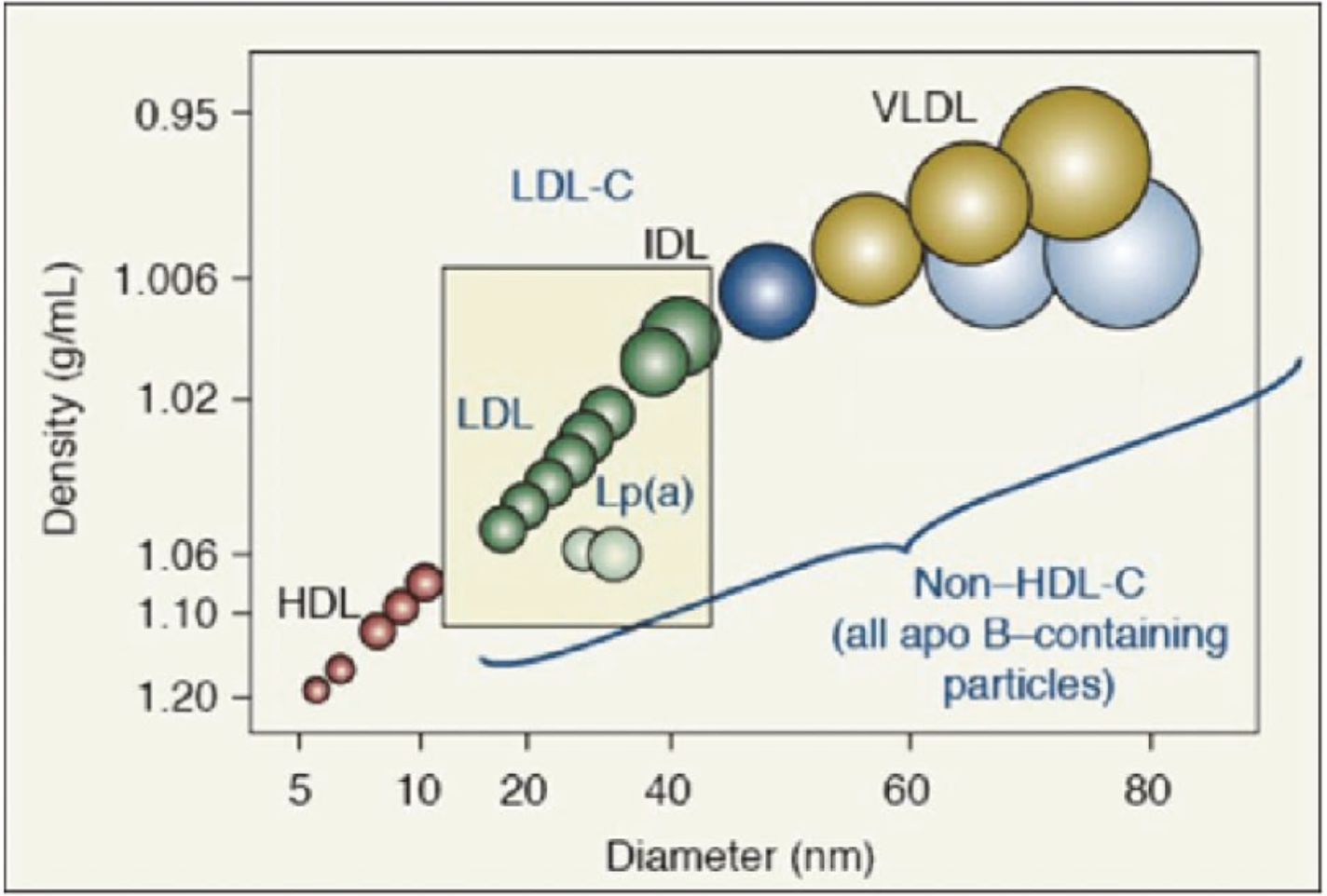
Gist: The key distinctions among these lipoproteins lie in their sizes and densities (i.e., ratio of lipid to protein). Figure 1 below also includes additional types of lipoproteins, which we will discuss in upcoming articles. Almost everything that is not HDL (i.e., non-HDL) in figure 1 is pro-atherogenic, meaning it can potentially promote the process that can lead to cardiovascular disease.
Atherogenesis (early stages) and atherosclerosis (later stages) are the disease processes that drive cardiovascular and cerebrovascular disease, which can result in conditions like stroke and heart attack, among others.
Nitty-Gritty: Interestingly, the core of all of these lipid particles is the same: varying amounts of cholesterol + triglycerides. It is specifically important to note that LDL and non-HDL particles can vary in size and density, and research has suggested that a higher number of small, dense particles may be more pro-atherogenic than larger, less dense particles. These smaller particles are more prone to oxidation and can more easily penetrate the lining of the arteries = damage and disease.
Luckily, these small, dense LDL and non-HDL particles have a marker on them: apoB. For every 1 of these small, dense LDLs and non-HDLs, there is 1 ApoB particle, therefore, the higher your apoB particle level, the greater the risk of disease. As 90-95% of apoB marked particles are LDL, I will just simply refer to LDL from here on out versus "LDL and non-HDL".
Gist: high apoB = higher cardiovascular risk.
So let's get this straight:
- The types of cholesterol are differentiated by their size and density (proportions of protein vs. lipid), whether they are LDL, HDL, VLDL and so on.
- Cardiovascular risk is generally assessed looking at your LDL (and non HDL-C) values. Our cholesterol blood tests gauge the concentration of different types of cholesterol, rather than the number of particles.
- When evaluating cardiovascular risk, it's the quantity of small, dense LDLs that are of most concern. Fortunately, these particles carry 1 apoB marker per LDL particle, therefore, allowing us to count them and then assign a level of cardiovascular risk based on the number present. This makes apoB a more direct indicator of cardiovascular risk.
My cholesterol is normal, why should I consider requesting an apoB level?
This apoB measurement can provide more accurate information about your cardiovascular risk compared to simply knowing the concentration of cholesterol within LDL (i.e. LDL-C value). Let's learn by example. ⬇️
Patient A and Patient B: As depicted in figure 3, both have the same LDL-C on their blood test, however, they do not have the same cardiovascular risk profile as we will see.
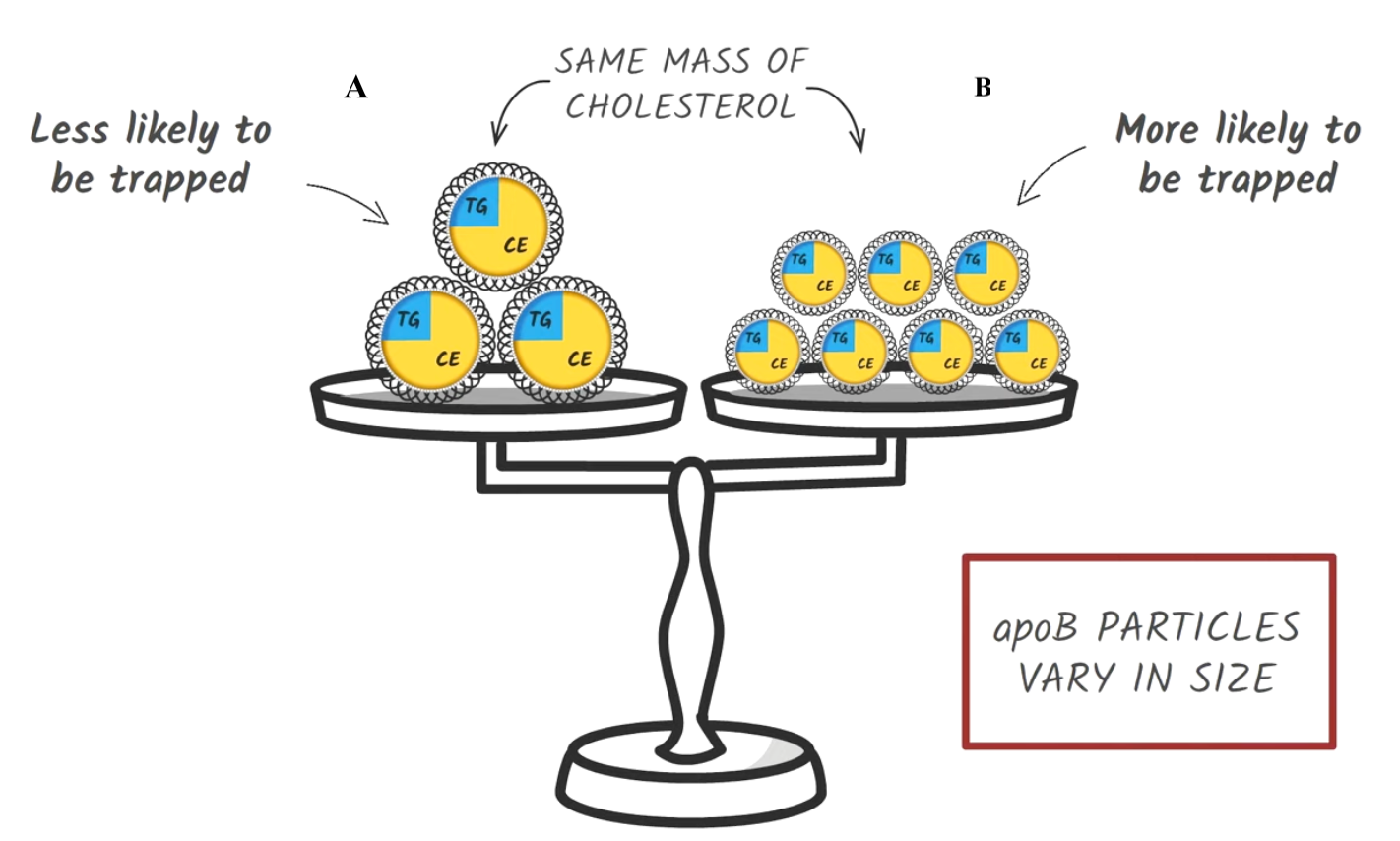
- Patient A has fewer, but larger LDL particles. The total density of cholesterol in these particles is high (because each particle is large), but there aren't as many particles, so the number of apoB molecules is relatively low. As we said, there is 1 apoB per LDL particle.
- Patient B has more numerous, smaller LDL particles. Each particle carries less cholesterol due to its size, but because there are so many particles, the total cholesterol density is the same as in Patient A. The apoB count, however, is higher because there are more LDL particles overall.
Gist: Even though both patients have the same LDL-C levels, Patient B is at greater risk for heart disease because they have more LDL particles, as indicated by a higher apoB count. The smaller LDL particles are more pro-atherogenic — they're more likely to get trapped in the arterial wall and contribute to plaque formation. This is why apoB can be a better predictor of cardiovascular risk than LDL-C alone. It takes into account not just the mass of cholesterol, but the number and size of the particles carrying it.
What do I do if I have a high apoB?
Managing high apoB often utilizes the same strategies we utilize to control high LDL-C. These include:
- engaging in regular physical activity
- adopting a heart-healthy Mediterranean-style diet
- maintaining a healthy weight
- refraining from smoking and excessive alcohol consumption.
If you find that your apoB level is high, the best first step is to consult with your health care provider. They can help you determine the most appropriate immediate actions and what additional interventions can be introduced over time.
Big Picture: In addition to the standard cholesterol panel, apoB can offer valuable insight into your cardiovascular risk, especially for individuals in situations similar to the patient example described in figure 3.
Are you still unsure about how this information applies to you or what your next steps should be? That's okay! During your next healthcare visit, request your cholesterol results and discuss them with your healthcare provider. The more knowledge you have, the more informed questions you can ask, enhancing your ability to actively participate in your health management.
Indeed, these topics can be complex and challenging– After all, if they weren't challenging, we'd have medicine all figured out and people would rarely get cardiovascular disease. However, it's our hope at TFP that articles like this one will foster meaningful discussions between patients and healthcare providers, enhancing understanding and promoting better health outcomes.
Sources and resources




 George Thanassoulis
George Thanassoulis
Disclaimer: The content provided on The Full Panel is for informational purposes only and is not intended to serve as a substitute for professional medical advice, diagnosis, or treatment. The information presented should not be considered or used as a replacement for personalized, expert advice from a healthcare professional.
While we strive to provide accurate, up-to-date, and relevant information, we make no warranties or representations about the completeness, reliability, or accuracy of the content presented. The information found herein may be subject to change without notice as medical knowledge and practices evolve over time. We strongly recommend consulting with a qualified healthcare professional before making any health or medical decisions.